


Corneal verticillata could be a sign of vision-threatening optic neuropathy
It isn’t every day that we notice something in the corneal exam that alerts us to the possibility of retinal disease, but it does happen. Classic examples:
Corneal arcus secondary to hypercholesterolemia, which increases the risk for intra-arterial plaques and other retinal vascular occlusions, and a non-healing and presumed neurotrophic corneal ulcer in a diabetic patient, indicating a high likelihood of retinopathy. And there are more subtle and less often encountered conditions that we should be aware of as well, namely corneal verticillata, or whorl keratopathy.
PRESENTATION
The condition presents as fine, grayish or yellow-brown, branching or whorl-like deposits, which often occur in a clockwise fashion within the interpalpebral cornea, making them distinct from other corneal findings.
Depending on the etiology, O.D.s should also look carefully for other ocular manifestations, such as lenticular opacities or retinal changes.
SYMPTOMS
Most of the time, these corneal changes do not impact vision, although patients may report photophobia and colorful halos around lights. Optic neuropathy would, of course, impact VA, although the patient could be asymptomatic initially.
CAUSES
Corneal verticillata is a commonly noted adverse effect of certain systemic medications — the most common are listed in Table 1 — whose properties cause them to bind to the cellular lipids within the corneal epithelium, basically causing a drug-induced lipid storage disease. Its corneal presentation is reversible with drug discontinuation.
|
|
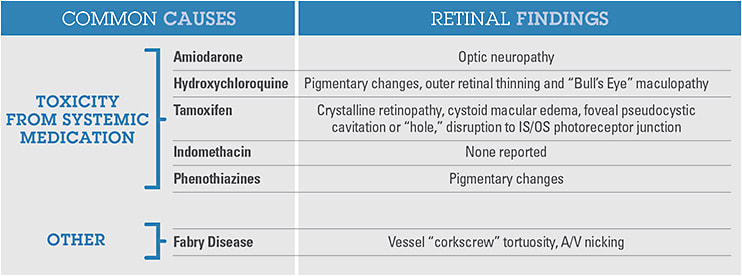
Just as these poorly metabolized drug particles end up in the cornea, they can work their way into the retinal structures (as described above). Amiodarone is the most common culprit. Because it is the most effective and most commonly prescribed anti-arrhythmic drug, O.D.s should be on the lookout for its use in cases of corneal verticillata, as well as irreversible central anterior subcapsular lens opacities and a less common, but vision-threatening, optic neuropathy. Essentially, all patients taking amiodarone will manifest whorl keratopathy within the first three months of treatment, but as early as within six days of use.
Amiodarone-associated optic neuropathy is thought to be due to an accumulation of lamellated inclusion bodies in the large axons of the optic nerve, reducing axoplasmic flow and leading to disc edema, according to the Journal of Clinical Neuro-Ophthalmology. It has an incidence of up to 2% and is 3.5 times more common in males. The incidence is higher in those with a longer duration of treatment, however, not related to dose, according to Ophthalmology. As opposed to a nonarteritic optic neuritis, or NAION, amiodarone-associated optic neuropathy tends to affect both eyes, manifests with a more gradual onset and takes longer to resolve. Most patients will eventually have some improvement in vision with medication discontinuation, however those with delay in diagnosis are at risk for severe and permanent vision loss.
In any case of corneal verticillata without a corresponding medication history, Fabry disease should be considered. Fabry disease is a multi-system genetic enzyme deficiency of alpha-galactosidase, which can also lead to lenticular opacities and retinal vascular abnormalities.
PATIENT EDUCATION
Reviewing findings and images with your patient serves to increase his engagement in his care, while also increasing compliance with follow-up visits. Corneal changes are fairly benign and, as such, are easy to present. An effective patient script:
“As you can see in this photo, there are grayish lines formed on the front surface of your eye, as a result of the medication you take for your atrial fibrillation. This is common and has not affected your vision. We’ll check again each year, so that if your vision or other symptoms change, we can work with your cardiologist to consider other options.”
On the other hand, optic neuropathy has a risk of vision loss and has the potential to have some other, more serious etiology.
“I found the cause of your blurry vision today to be swelling in your optic nerves, which occasionally occurs as a result of the amiodarone you take. Further testing to confirm the cause, including blood tests and brain imaging, may be needed. It’s important that we reduce the swelling as quickly as possible, so that it does not lead to permanent vision loss. We will consult with your cardiologist about possibly discontinuing the medication, and may also need to prescribe additional medications. We will see you back in two weeks for further testing and follow up.”
DUE DILIGENCE
A typical eye exam is performed in sections: refractive assessment, anterior segment, then posterior segment. As such, we tend to examine individual structures as separate entities. That said, we know from our anatomy courses and from our inherent knowledge of the eye that the structures are, of course, related. Optometrists should always keep this, and the eye’s connection to the body, in mind when performing eye examinations of any kind. OM
