


Tips and tricks for successful, happy patients
The fitting of scleral lenses is an option that is truly life changing for patients who have corneal irregularities, ocular surface issues and issues with other lens designs. Fitters acquiring these skills today have access to, what seems to be, unlimited resources to assist the fitting pro-cess, but one aspect that is still incredibly challenging is teaching lens insertion.
Due to the diameter of the lens, and the limitations of the palpebral fissure, special attention is required when teaching lens insertion techniques. Despite all their advantages, scleral lens insertion proves to be one of the most challenging aspects of this solution and can lead to patient dropout. To be successful, the insertion process requires necessary attention, and sometimes a few tricks. Let’s first review the “textbook” methods of teaching and then see whether we have any other education for our more challenging patients.
TEXTBOOK METHOD
Traditional methods of scleral lens insertion include placing the lens on a plunger or use of a three-finger support technique. Both methods require the patient to be sitting or standing and using a flat mirror. After filling the lens with the recommended solution, the patient is encouraged to lean over the mirror, use their index finger to secure the upper lid and the middle finger to secure the lower lid, and then gently place the lens into the eye.
While all that sounds easy, any fitter will tell you that some patients find this extremely challenging. So, what options do we have when the patient just can’t insert the lens?
TIPS AND TRICKS
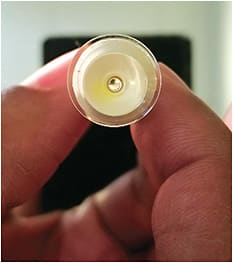
Cut the plunger. When a patient loses fixation during insertion, this sometimes causes a Bell’s phenomenon. This is when the eye rolls up, making lens insertion next to impossible. Methods used to maintain fixation, such as using a ventilated plunger, can help combat this phenomenon. Cutting the bottom of the plunger allows light to pass through it, creating an excellent fixation target for the patient (Figure 1).
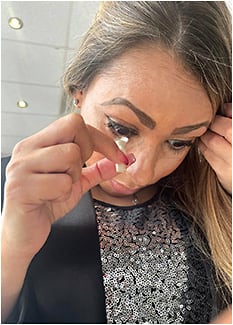
Hands-free approach. For new contact lens wearers, the idea of having a large diameter lens in the eye can be quite intimidating. In these patients, it is common to have an aggressive blepharospasm response as the lens approaches the eye. One way to address this is to allow the patient to use both hands. Several stands can be purchased to outfit this, some of which contain fixation lights. However, a simple option is popping a hole in a paper cup (Figure 2).

Insertion bubbles. Air bubbles present a challenge because these can affect vision and comfort. When present, the lens must be removed and reapplied. Bubbles are often the result of the angle of insertion. When inserting, if the head is slightly titled back, this will cause air to be trapped between the lens and the eye. To rectify this, have the patient physically feel themselves tucking their chin into their chest. This will greatly assist with the angle of insertion (Figure 3). If this angle persists as a problem, overfilling the insertion solution or using a thicker insertion solution (non-preservative) may help solve this problem.
OVERCOME INSERTION TROUBLES
Scleral lenses offer too many benefits to let something like insertion troubles discourage our patients. Like everything else we do, identifying the specific issues our patients have and combating them with unique responses will increase our opportunity for success. OM
