


Align optics for more successful outcomes in fitting multifocal contact lenses
Innovation in multifocal contact lens designs and materials, as well as expansion of modalities and prescriptions, continues to drive success in meeting the contact lens needs of presbyopes. Challenges remain, however, for a subset of patients who do not achieve the level of visual quality they desire, despite multiple attempts at fitting.
Various factors affect patient success and satisfaction with bifocal and multifocal contact lenses. These include pupil size, optics, neural adaptation and tear film stability.1
In evaluating multifocal contact lenses on the eye, an additional key fitting consideration is optical alignment. Haloes, monocular diplopia and ghosting have been attributed to the misalignment of the contact lens optics with the visual axis.2,3 Three potential causes of misaligned optics are lens decentration, pupil position and angle kappa.
Here, we’ll discuss how to assess optical alignment and account for potential causes of misalignment.
ASSESS OPTICAL ALIGNMENT
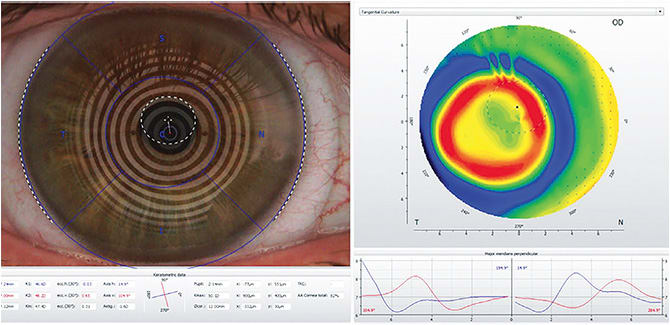
A direct and simple method for evaluating a misalignment between the center of the multifocal optics and a patient’s visual axis is to compare topography taken on the bare cornea to the topography taken with the contact lens on the eye. Display the tangential power maps, and use the topographer’s “difference display” map setting, (also known as subtractive or comparative maps), which subtracts the map taken over the top of the contact lens from the baseline map. Measure the difference between the patient’s visual axis (center of map) and the center of the multifocal optics by using the topographer’s measuring tool.
POTENTIAL CAUSES OF MISALIGNMENT
Contact lens decentration. The centration of soft and scleral contact lenses, both fit to land on the conjunctiva just beyond the limbus, is largely influenced by the shape of the anterior ocular surface. We may observe temporal decentration of soft contact lenses (up to 1 mm) and inferotemporal decentration of scleral contact lenses (about 0.84 mm inferiorly and 0.55 mm temporally).3,4 This can be explained by the non-rotationally symmetric shape of the ocular surface beyond the cornea, with the nasal region being more elevated (flatter) compared to other quadrants.5 Despite best attempts to achieve perfect centration by altering soft lens diameter and/or customizing scleral haptics, this is not always achievable.
Pupil position. Most patients’ pupils are decentered in the superior nasal direction within the iris, opposite to the aforementioned temporal decentration of contact lenses. Given the prevalence of small pupils in presbyopes, we can understand that the position of the pupil relative to the contact lens optics is an important factor in the visual outcome when fitting multifocal contact lenses.6
Angle kappa. Angle kappa is the angle between the visual axis (line connecting the fixation point with the fovea) and the pupillary axis (line that perpendicularly passes through the entrance pupil and the center of curvature of the cornea). The light reflex is near the visual axis at the corneal plane. The average angle kappa is about ±5°. Hyperopic patients tend to possess larger angle kappa values, which may result in increased glare when the contact lens optics are not properly aligned with the line of sight.7 Taking from advances in refractive and cataract surgery, we have witnessed that compensating for angle kappa, by offsetting the contact lens optics, plays a measurable role in patient satisfaction.7
ACHIEVE ALIGNMENT WITH OFF-SET OPTICS
While individual patient sensitivity to optical misalignment varies, studies show incorporating from 0.2 mm to 0.4 mm or more of offset optics in multifocal contact lens designs to be of benefit in optimizing clinical outcomes.6 Several manufacturers offer this important parameter of customization in both soft and scleral lens designs.
As we, as optometrists, strive for greater success in meeting the needs of the growing presbyopic population, we look toward these and future advances in optical design. OM
REFERENCES
- Remón L, Pérez-Merino P, Macedo-de-Araújo RJ, Amorim-de-Sousa AI, González-Méijome JM. Bifocal and Multifocal Contact Lenses for Presbyopia and Myopia Control. J Ophthalmol. 2020. doi.org/10.1155/2020/8067657
- Ramdass S, Norman C, McCorkle L, Lampa M. Objective & subjective visual response to decentered multifocal optics. Poster presented at the Global Specialty Lens Symposium; Jan. 25-28, 2018. Las Vegas.
- Cox I. Kollbaum P, Papas E. Advances in optics drive soft lens success. Review of Contact Lenses. March/April 2021:20-25.
- Kowalski LP, Collins MJ, Vincent SJ. Scleral lens centration: The influence of centre thickness, scleral topography, and apical clearance. Cont Lens Anterior Eye. December 2020 43(6):P562-567 doi.org/10.1016/j.clae.2019.11.013
- Ritzmann M, Caroline PJ, Boerret R, Korszen E. An analysis of anterior scleral shape and its role in the design and fitting of scleral contact lenses. Cont Lens Anterior Eye. April 2018 41(2):205-213. Doi:10.1016/j.clae.2017.10.010.
- Walker M, Caroline P. Soft Lens Centration Based on Scleral Shape Measurement. World Wide Vision XV. Soft Special Edition website. http://softspecialedition.com/world_wide_vision_xv . Accessed July 12, 2021.
- Kumar DA, Agarawal A, Jacob S. Angle kappa may play important role in success of multifocal IOLs. Ocular Surgery News. May 10, 2010.
