


For hundreds of years, presbyopia has been corrected with bifocals, thanks to Benjamin Franklin’s strained sight and knack for problem solving. The possibilities for correcting near vision have expanded rapidly since that 1784 invention. (See “Worldwide Prevalence of Presbyopia by Region,” p.24.)
Here, those who regularly see presbyopic patients discuss the different options and how to determine the best recommendation. (See “Unaddressed Refractive Errors Worldwide,” p.26.)
CONTACT LENSES
Lisa Greene, OD, of Asheville Vision and Wellness, in North Carolina, says she has a strong base of patients wearing contact lenses, such as multifocals, for their long-arm syndrome.
“The lenses today help keep the eye moist and imitate the corneal surface, so that patients don’t feel them,” she explains.
She adds that she prescribes monovision contact lenses for patients considering LASIK, so they can get an idea of what to expect from their vision.
Ideal patients. Dr. Greene says current contact lens wearers and brand-new presbyopes are the ultimate candidates because they are already experienced wearers, and the latest lenses provide exceptional comfort, respectively.

OPHTHALMIC LENSES
In addition to bifocals, this presbyopia treatment category is comprised of reading glasses and progressive lenses.
Ideal patients. “If presbyopia is the patient’s first vision problem, over-the-counter readers make a lot of sense because they are simple and inexpensive,” offers Jacob Lang, OD, FAAO, lead optometrist at Associated Eye Care, in Stillwater, Minn. “When you start there, you can always work your way to different options over time. Early presbyopes may only need readers for certain situations, such as reading medication labels, threading a needle, or tying fishing line. But if they start to progress to a more substantial portion of their day being impacted by visual problems, then we can talk about other options.”
Mark R. Kapperman, OD, of Kapperman, White & McGarvey, in Chattanooga, Tenn., says presbyopes who work on computers and perform close work are ideal candi-dates for progressive lenses, which contain corrections for both.
“Computer or ‘office’ progressive lenses have gotten a lot better, in that the wearer no longer has to bob their head to find their needed vision,” he explains. “I have found these lenses make a great choice for someone who is doing a lot of desk work.”
Worldwide Prevalence of Presbyopia by Region1
PRESBYOPIA DROPS
Nate R. Lighthizer, OD, FAAO, associate dean at NSU Oklahoma College of Optometry, in Tahlequah, Okla., says he’s excited about this recent addition to the treatment toolbox because they give presbyopia patients another option to try.
Vuity (AbbVie) is currently the only FDA-approved drop. It is comprised of 1.25% pilocarpine hydrochloride and a proprietary vehicle to constrict the pupil and contract the ciliary body. Seven other drops are in the pipeline.
Ideal patients. Dr. Lighthizer believes this is the patient who has never needed visual correction, using himself as an example.
“In the next three-to-five years, I’m likely to start noticing some near vision blur,” he points out. “As someone who has never had a prescription and has never had to wear glasses, the eye drop is appealing to me. Also, I am not near cataract age, so drops are a good in-between option before I reach the point where I need surgery.”
Dr. Lang says he thinks presbyopia drops may be a good choice for patients who are a bit further along in their presbyopic journey.
“As these patients find that more of their daily vision is broken, the drops might be appealing, so that they don’t feel they have to wear readers as often,” he offers.
Jade Coats, OD, who practices at McDonald Eye Associates, a multi-location practice, in Fayetteville, Ark., says she thinks the ideal patient for this treatment option is the presbyope who wants an adjunct treatment to their current solution, as the drops’ mechanism of action is temporary.
“The big question for presbyopia patients is, ‘Do you want glasses, contact lenses, or refractive surgery?’” Dr. Coats says. “Then, we can talk about how to use the drops to make one of those options even better.”
SURGICAL OPTIONS
These treatment options are corneal inlays, laser surgeries (conducive keratoplasty, LASIK, LASEK, and photorefractive keratectomy), and premium IOLs.
Ideal patients. “Surgery-associated options are typically a consideration for patients who either don’t want to wear glasses or contact lenses or have been dissatisfied with the vision provided from either,” says Dr. Coats. “These patients also make excellent candidates because their dislike of these vision appliances is a motivating factor to succeed in surgery-associated options. Still, there are always risks associated with surgery, so despite how gung-ho a patient may appear, these risks must be discussed, so the patient knows precisely what could occur.”
Dr. Kapperman agrees with Dr. Coats.
“It is always important to help patients understand the risks vs. the benefits of a laser procedure. There are many happy laser surgery patients out there, but pre-surgical patients need to be informed that it will not prevent presbyopia from naturally progressing,” he points out. “Therefore, they should have an understanding that, over time, they often still need to wear reading glasses.”
The benefit of corneal inlays, which use the “pinhole effect” to help focus light, enabling the wearer to see up close, is that they are removable, meaning the patient isn’t locked into the inlay, if it doesn’t meet their visual expectations, Dr. Kapperman notes.
For presbyopic patients requiring cataract surgery, presbyopia-correcting IOLs can be ideal, say those interviewed.
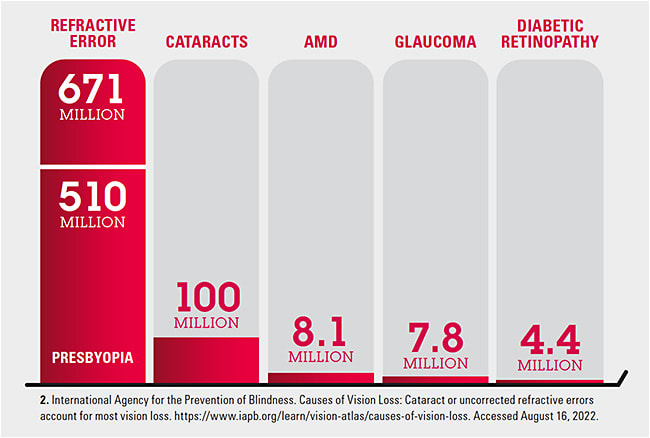
Unaddressed Refractive Errors Worldwide2
DETERMINING THE BEST RECOMMENDATION
While there is an ideal patient for each option in the presbyopia treatment toolbox, it’s important to obtain a thorough patient history and a description of the patient’s lifestyle to increase the likelihood of success, say those interviewed.
“Our techs do a nice, thorough history during the patient workup, so that we can look at how the patient uses their eyes on a day-to-day basis,” Dr. Kapperman explains. “Do they stare at a computer all day long? At what points are they experiencing the most visual trouble? I also ask a lot of probing questions during my exam that feed into the decision-making process.”
He adds that part of this history is finding out what current and/or prior refractive correction devices (i.e., glasses, contact lenses) or surgeries these patients have tried to see what treatment option the patient may be most comfortable with.
“Most of the time, patients are comfortable sticking with what they already know,” he asserts.
Dr. Lang agrees.
“You aren’t likely going to get a patient who is currently in glasses to suddenly switch to contact lenses just because they’ve developed presbyopia,” he says.
THE MORE, THE MERRIER
It can be argued that too many options can be overwhelming, but not when it comes to treating presbyopia, say those interviewed.
“Since every patient is different, the more options we have, the more likely we’ll be to tailor a solution to each individual,” Dr. Lighthizer says. “And we all know that a happy patient is a happy practice.”
Dr. Lang concurs.
“There is no cure for presbyopia, so the more options optometrists can have in their treatment toolbox, the better,” he says. “Patients are not always thrilled to talk about presbyopia, but with more corrective options than ever, it’s an easier conversation.” OM