


This article was originally published in a sponsored newsletter.
This case presentation highlights the complexities of managing advanced glaucoma in a 63-year-old male patient who was referred to the Glaucoma Institute of State College in State College, Pa.
Presenting Signs:
- Uncontrolled intraocular pressure (IOP): Despite brimonidine and timolol bid use, IOP remained elevated at 23.7 mm Hg and 21.8 mmHg.
- Grade 2 cataracts: Vision was correctable to 20/25, but cataracts contributed to glare and reduced vision (20/50).
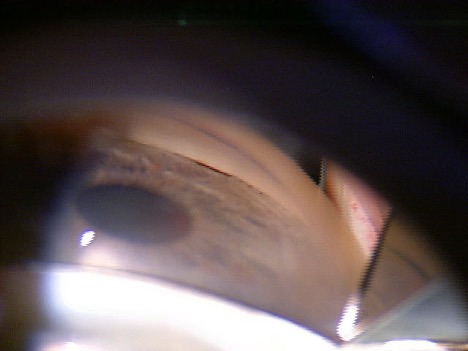
- Gonioscopic findings: Posterior trabecular meshwork was barely visible in all four quadrants with peripheral anterior synechiae, potentially hindering outflow pathways (Figure 1).
- Central corneal thickness (CCT): Pachymetry values of 523 μm and 528 μm suggested a thin cornea, which could influence IOP readings.
Diagnosis:
- Primary angle closure glaucoma.
Diagnostic and Management Challenges:
- CCT and IOP readings: True IOP may be underestimated when corneas are thin. Corneal compensated IOP calculation or alternative measurement techniques might be necessary.
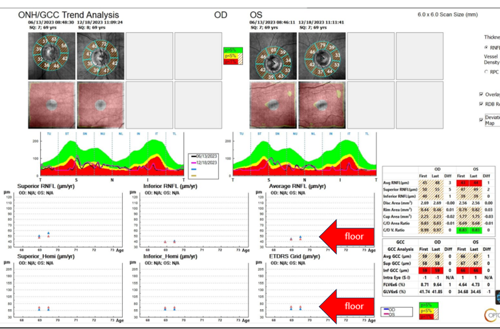
- The OCT floor effect: This patient was below floor on both ganglion cell complex and nerve fiber layer, which made serial OCT interpretation more challenging (Figure 2).1
- Visual field (VF) testing: VF testing in advanced glaucoma is affected by reduced reliability and reproducibility.2
Solutions:
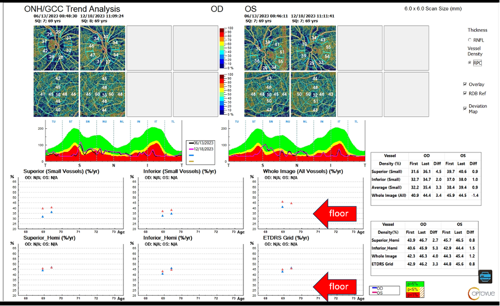
- Optical coherence tomography angiography (OCT-A): OCT-A has a much lower floor with circumpapillary capillary density of 31.2% and perifoveal vessel density around 28%. Practically, this means that using OCT-A is suited to monitoring future progression vs. conventional OCT (Figure 3).2
- Visual fields: These tests were employed to look for new defects or widening of existing defects. Monitoring the deepening of existing defects was much less helpful because the dynamic range ended around 15 to 19 dB. We should also consider 10-2 or MTOP testing strategies in such cases.3-4
Treatment:
- The patient underwent successful cataract surgery with goniosynechialysis and Kahook dual blade goniotomy OU. His IOP is now in the mid-teens.
Reference(s):
- Moghimi S, Bowd C, Zangwill LM, et al. Measurement floors and dynamic ranges of OCT and OCT angiography in glaucoma. Ophthalmology. 2019 Jul;126(7):980-988. doi:10.1016/j.ophtha.2019.03.003
- Russell RA, Garway-Heath DF, Crabb DP. New insights into measurement variability in glaucomatous visual fields from computer modelling. PloS One. 2013 Dec;8(12):e83595. doi:10.1371/journal.pone.0083595
- Artes PH, Hutchison DM, Nicolela MT, LeBlanc RP, Chauhan BC. Threshold and variability properties of matrix frequency-doubling technology and standard automated perimetry in glaucoma. Invest Ophthalmol Visual Sci. 2005 Jul;46(7):2451-2457. doi:10.1167/iovs.05-0135
- Gardiner SK, Swanson WH, Goren D, Mansberger SL, Demirel S. Assessment of the reliability of standard automated perimetry in regions of glaucomatous damage. Ophthalmology. 2014 Jul;121(7):1359-69. doi:10.1016/j.ophtha.2014.01.020
