


This article was originally published in a sponsored newsletter.
Our areas of expertise differentiate our practices and make us successful. I see a significant number of urgent and emergent anterior segment cases, but for the most part, my expertise is in the back of the eye. One of the more common conditions I see is diabetic retinopathy, especially in patients I have had the pleasure of seeing for many years. In some cases, patients have a long history of diabetes with minimal or no retinopathy, whereas other folks have a significant number of complications related to diabetic retinopathy. Early center-involved diabetic macular edema can be difficult to visualize in vivo at the slit lamp, but the presence of refractile exudates involving the fovea can make visualization easier. In other cases, the foveal avascular zone looks relatively benign, while visual acuity is affected.
These nuances in presentations can be complicated by imaging if scans are taken in different locations. In Figures 1 and 2, we see two sets of OCT scans of a patient with center-involved macular edema. In both images, the reference or baseline scan is in August and the follow-up scan is three weeks later. The difference between Figure 1 and Figure 2 is the location of each set of scans: they are located adjacent to each other.
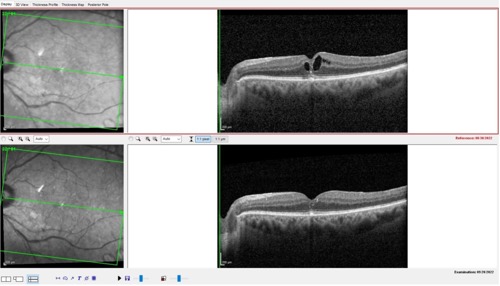
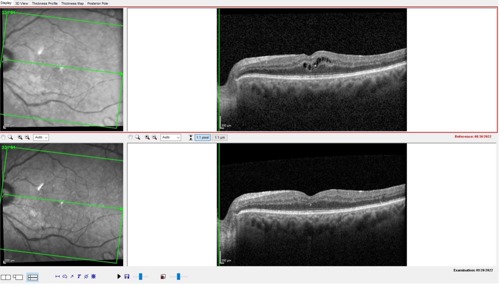
Note that in Figure 1, the scans were taken through the center of the fovea; whereas in Figure 2, the scans were taken a few microns above the center of the fovea. It is important to note that even though these two (top) scans were taken close together, there is marked difference in the appearance of the intraretinal fluid in each scan.
One distinct advantage of the Spectralis (Heidelberg) is its ability to register images from baseline to all follow-up scans. The baseline image is registered as the reference image, and follow-up scans are taken in exactly the same location. This function is important in determining progression or improvement of a disease process. For example, let’s say these images were not registered. If the upper image in Figure 1 was the first scan, and an unregistered follow-up scan was obtained in the location seen in Figure 2, it would appear as though the condition improved. The reverse would be true if Figure 2 was the baseline and Figure 1 was the follow-up: The condition would appear to have worsened. In reality though, you would essentially be comparing two different scan locations, not the same scan location, which would make it difficult to determine progression or improvement.
By employing image registration for follow-up scans, we can see exactly what is happening in the exact same location on follow-up visits. In this case, we can see clearly that the center-involved edema has decreased in both scan locations and, therefore, the condition is improving. How do you know if your images are registered? Most of the time, the choroid gives us the clue. In diabetic macular edema, the choroidal vasculature is not involved to the extent that the anterior retinal circulation is, and a close examination of the choroidal vessel architecture in a baseline scan should reveal the same exact picture of the choroidal vasculature in the follow-up scan. If the choroidal vasculature looks different, the scans are in a different location.
Scan location is critical to determining improvement or worsening of a condition. The Spectralis takes the guesswork out of the clinical decision-making process, resulting in better clinical care and outcomes.
