



The discernment between glaucoma and the many non-glaucomatous optic neuropathies (NGONs) is a challenge. (See “Table 1: List of NGONs” p.13.) This is because the latter have been reported to cause optic nerve cupping, which mimics glaucoma. A misdiagnosis can lead to testing and treatment that isn’t needed and may have a negative effect on the patient’s sight and systemic health (e.g., an intracranial tumor). Therefore, optometrists must strive to differentiate glaucoma from NGONs.
This article provides a systematic approach to accurately distinguishing glaucoma from NGONs. This approach is comprised of acquiring a case history, medical and family history, patient’s medication use, review of systems, and a comprehensive exam.

Case history
Listening attentively to any symptoms, such as changes in vision, pain, or visual disturbances, as well as determining condition onset and progression are the first steps to proper diagnosis:
• Symptoms. We know that glaucoma is referred to as the “silent thief of sight” due to its slow progressive nature without significant noticeable symptoms. Depending on the amount of glaucomatous damage, patients can present with a variety of symptoms, some of which may be similar to that of other ocular conditions (e.g., cataract, and corneal disease). Specifically, the symptoms may be cloudy vision, peripheral visual field (VF) decline, patches of an image missing, or vision decline. I have found that patients who can describe their glaucomatous symptoms are likely to be in the moderate-to-advanced stages of the disease.
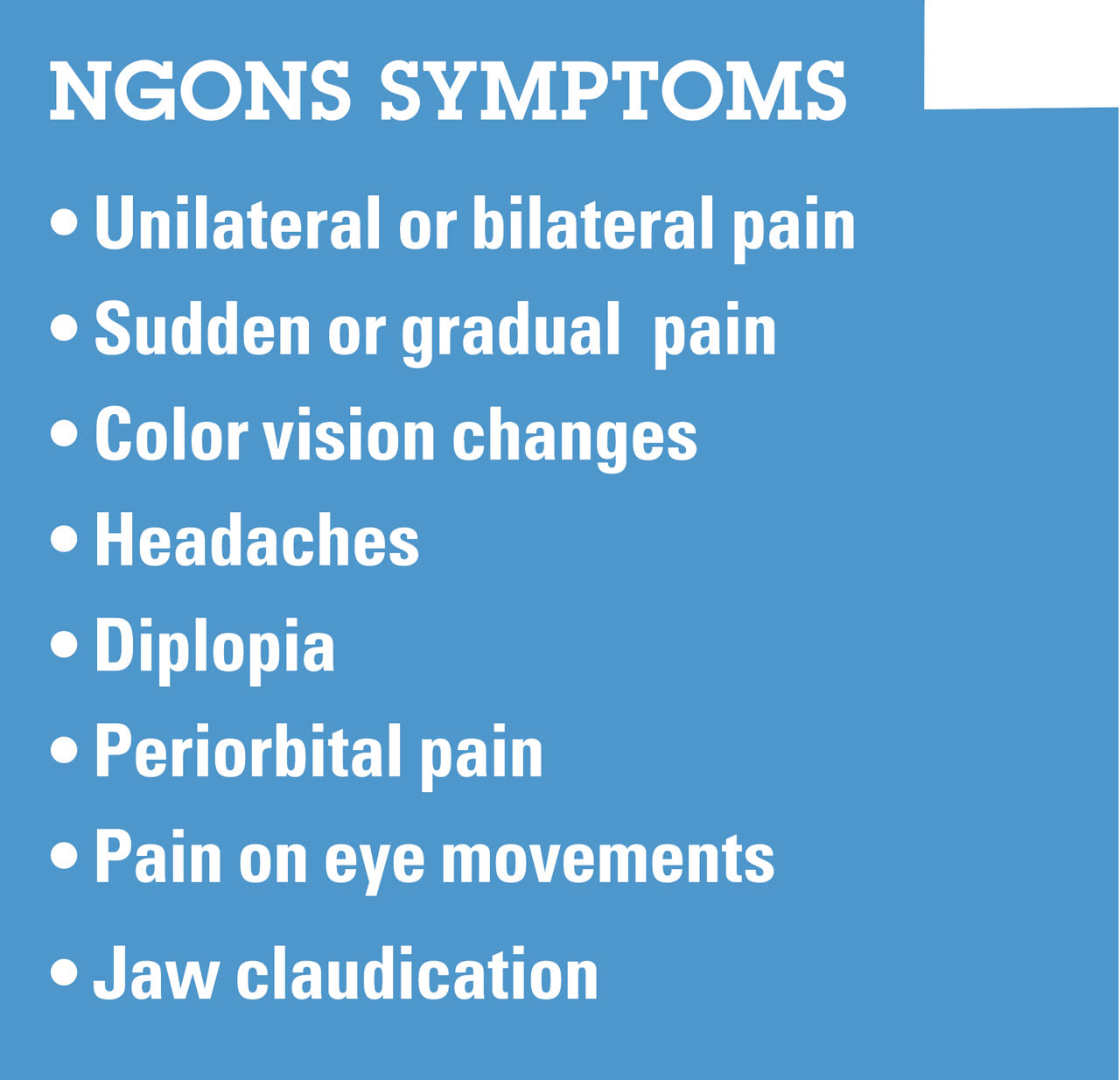
NGONs, on the other hand, can manifest in various ways. For example, optic neuritis presents with acute pain upon eye movement, color disturbances, and/or rapid vision loss. What’s more, ischemic optic neuropathy may result in sudden, painless vision loss. (See “Table 2: NGONs Symptoms.”)
• Onset and progression. Glaucoma commonly has a slow, gradual decline. NGONs often present as sudden onsets of symptoms, such as a decline in vision or VF over hours to days and, in some cases, are accompanied by other symptoms. Optic atrophy due to optic neuritis is an example. It can present with vision loss accompanied by blurry vision, pain from eye movement, and decrease in contrast.
Medical/family history
In the case of the “silent thief of sight,” a positive family history increases the risk of open-angle glaucoma.1 Additionally, patients who have conditions such as hypotension, sleep apnea, Raynaud’s syndrome, and Flammer syndrome are at a high risk for low-tension glaucoma.2 Thus, these histories can point toward a glaucoma diagnosis.
In the case of NGONs, autoimmune conditions, such as myasthenia gravis, rheumatoid arthritis, inflammatory bowel disease, ankylosing spondylitis, sarcoidosis, systemic lupus erythematosus, Sjögren’s syndrome, and Wegener’s granulomatosis, may increase the risk of NGONs.3 Further, vascular disorders, such as diabetes and hypertension, may also increase NGONs’ risk. Therefore, patients who have optic atrophy and these histories should raise suspicion for a NGON.
Medication use
Certain medications, such as corticosteroids, can increase IOP, potentially exacerbating the chance of developing open-angle glaucoma. Additionally, the use of topical or systemic adrenergic agonists, such as phenylephrine, can lead to angle-closure glaucoma due to pupillary block.4 Thus, the use of these medications in the proper clinical setting may indicate the presence of glaucoma.
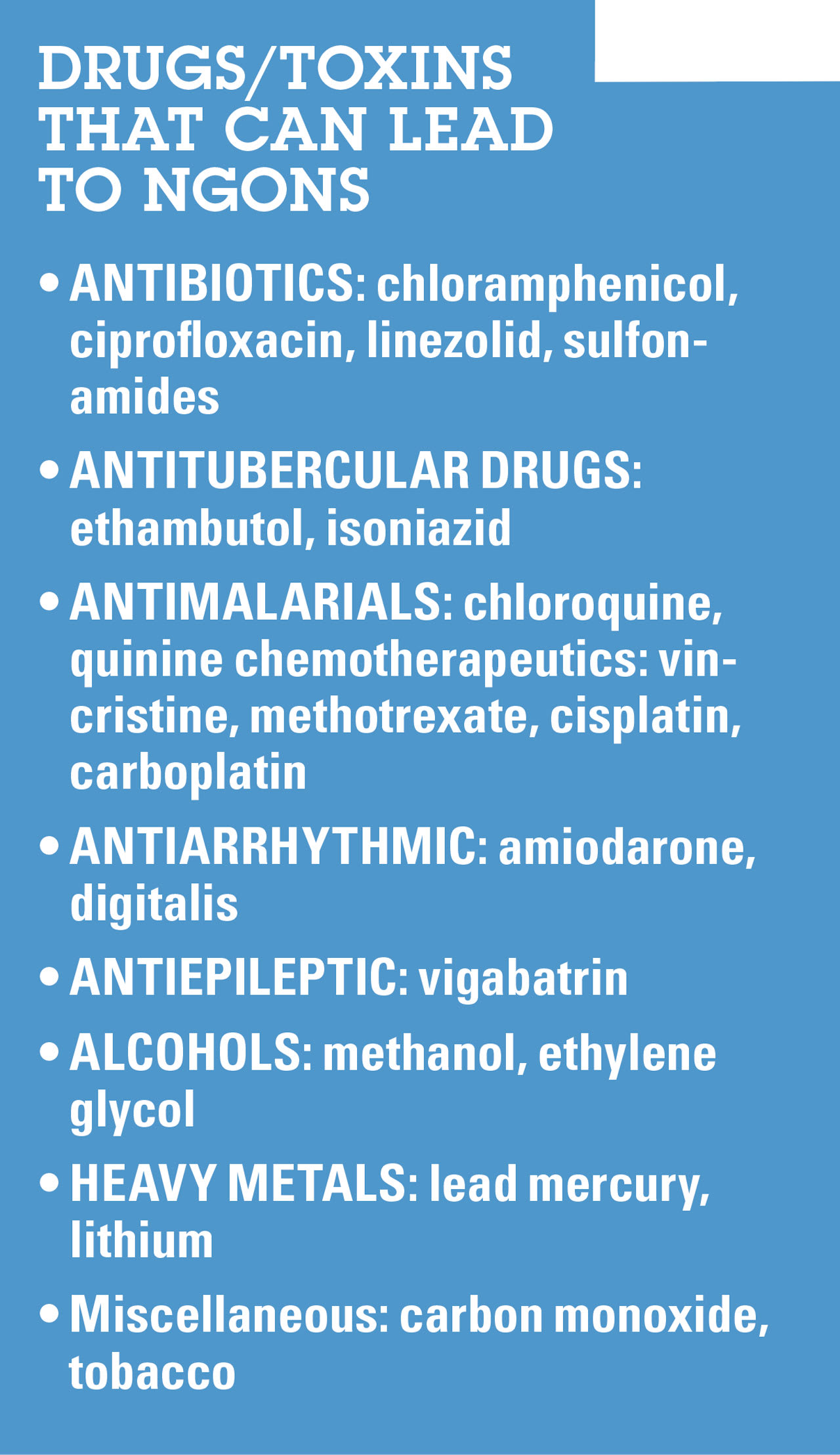
Several drugs, such as anti-leptics, and toxins, including antibiotics, and heavy metals, respectively, can lead to NGONs.5,6 Therefore, these compounds can signal a NGON. (See “Table 3: Drugs/Toxins That Can Lead to NGONs.”)
Review of systems
A comprehensive review of systems can help identify potential systemic conditions that may contribute to glaucoma or NGONs. As examples, sleep apnea may lead to glaucoma through low ocular perfusion, and conditions, such as multiple sclerosis and thyroid eye disease, can lead to NGONs through inflammation and compression, respectively.
Comprehensive exam
This is comprised of these areas:
• VA assessment. Central vision is usually preserved until the advanced stages of glaucoma. NGONs, on the other hand, can lead to a wide variety of VA outcomes. As an example, VA in non-arteritic anterior ischemic optic neuropathy (NAION) patients may range from 20/20 to hand motions or worse. Additionally, a change in central vision without a past indication of glaucoma can be associated with NGONs.
• Dilated pupillary examination. Pupils typically react normally in glaucoma, with no relative afferent pupillary defect (RAPD), due to the bilateral nature of glaucoma. That said, RAPD may be present in uncommon cases of advanced unilateral or asymmetric glaucoma. In the case of unilateral or asymmetric NGONs, a RAPD in the affected eye can be noticed.
• Red cap desaturation test. As with pupil examination, this subjective test reveals normal results in most patients who have bilateral glaucoma, unless the condition is significantly asymmetric. Additionally, this test can aid in confirming asymmetry of damage between glaucomatous or non-glaucomatous optic atrophy. About 25% of healthy adults notice desaturation with an average intraocular difference of 10%.6
• Pachymetry. Even though elevated IOP is considered the hallmark for the development and progression of glaucoma, we must remember that a significant number of glaucomatous cases present with IOPs in the normal range.5 IOP value must be considered with respect to the patient’s pachymetry values. Pachymetry values of less than 555 µm indicate an underestimation of IOP. In fact, the risk for glaucoma doubled for every 40 µm decrease in corneal thickness, according to one study.5 For this reason, when considering a glaucoma diagnosis, we should acquire the patient’s pachymetry values during the initial workup.
• Slit lamp exam. A thorough and careful slit-lamp assessment is essential when suspecting glaucoma. This is because the slit lamp exam can reveal the clinical signs of the silent thief, such as Krukenberg’s spindle, pseudoexfoliation material on the lens and pupillary margin, and any anterior chamber reactions. Evaluating angles through the slit lamp and confirming with gonioscopy or anterior segment (AS) optical coherence tomography (OCT) is essential for the accurate classification and effective treatment of glaucoma. NGON would not have such findings.
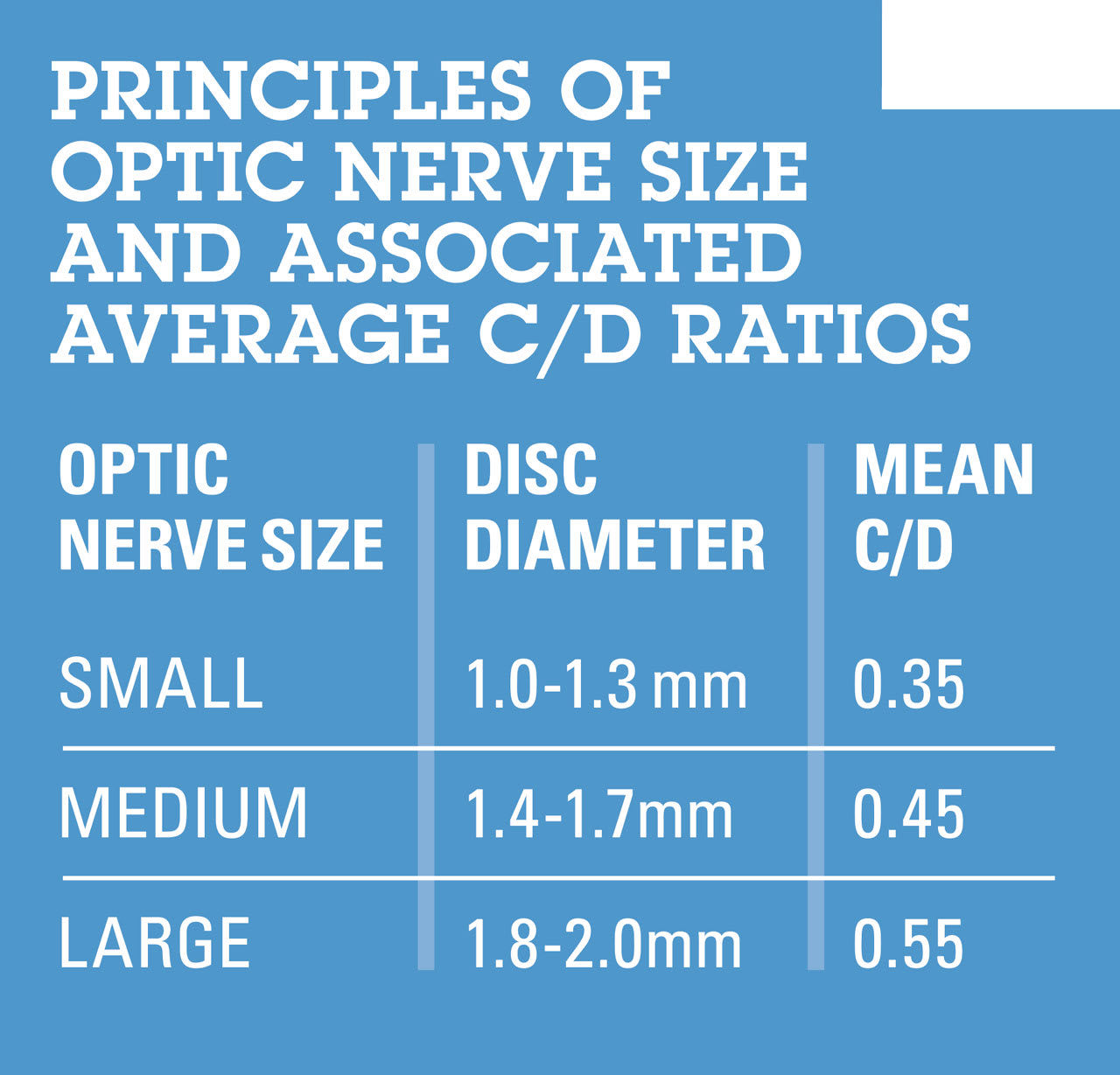
• Optic nerve evaluation. (See Table 4: Principles of Optic Nerve Size and Associated Average C/D Ratios.") Glaucoma is often simplified as a condition of high cup-disc ratio (C/D ratio): The larger the optic nerve size, the larger the C/D ratio.7 (See “Table 4: Principles of Optic Nerve Size and Associated Average C/D Ration.") Analyzing the C/D ratio without proper context is like analyzing IOP without pachymetry values, in that the data are incomplete. The quality is more important than the quantity (C/D ratio) when looking at the optic nerve. Thus, when assessing the optic nerve and its surrounding area, we must consider elements, such as optic nerve size, color of the rim, presence of focal rim defects or notching, parapapillary atrophy, defects in the retinal nerve fiber layer (RNFL), and disc hemorrhages to help discern glaucoma from a NGON.
The Greenfield criteria aids in identifying when it’s recommended to order neuroimaging in patients who have optic neuropathies. Specifically, the criteria are patients younger than age 50, with VA below 20/40, and who display more pronounced optic nerve pallor than cupping, and exhibit vertically aligned VF defects.8
Clinicians use the inferior ≥ superior ≥ nasal ≥ temporal, or ISNT, rule to remember the normal appearance of the optic rim. This can help detect any area that might differ from the rule to catch early glaucomatous changes.
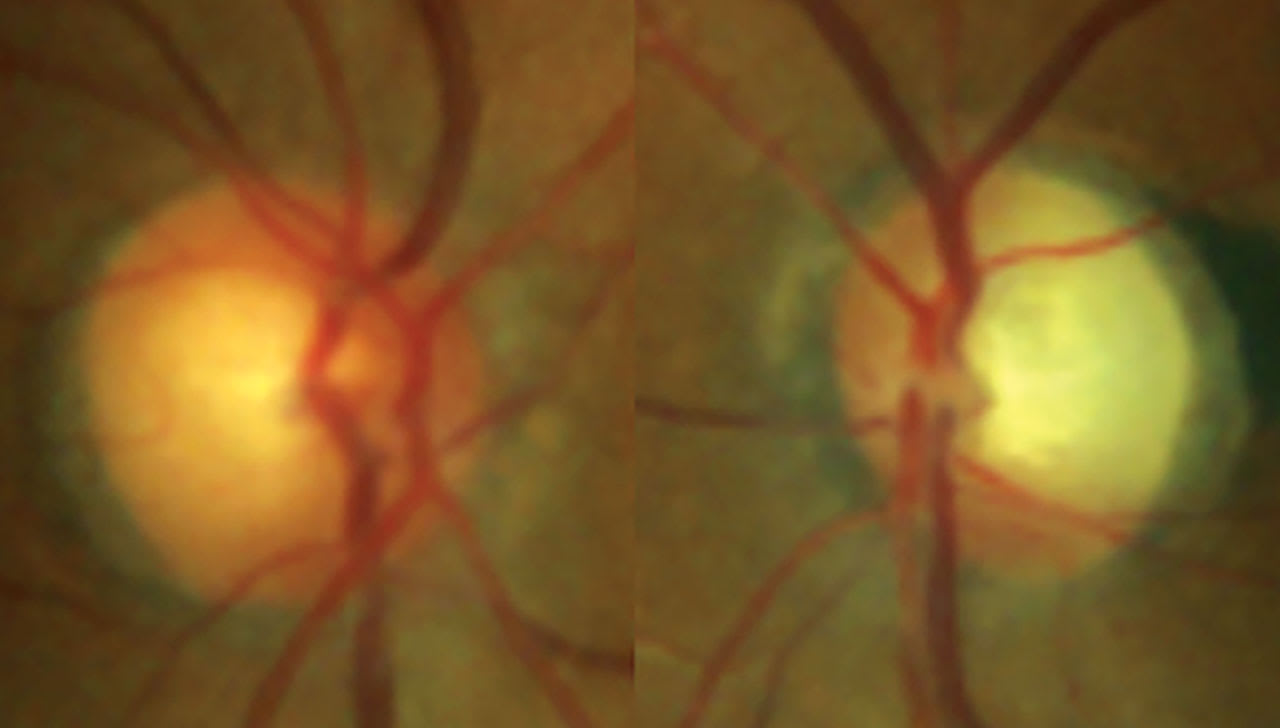
Pallor of the optic rim is a cardinal sign for NGON. The pallor can be diffuse, as seen in arteritic anterior ischemic optic neuropathy (AAION) or sectoral, often seen in NAION. Patients who have a NGON can present with cupping, in addition to pallor. Noticing pallor during a dilation exam can often be dependent on clinical experience. Obtaining baseline fundus photographs makes monitoring the pallor easier, so we can assess intraeye and intereye pallor that extends beyond the cupping. An advance glaucomatous nerve may appear pale due to exposure of scleral tissue, but even then, it has perfusion, unlike in NGONs.
Other clinical signs of glaucoma include disc hemorrhages, which are a sign of disease pro-gression and most often found inferiorly temporal and superiorly temporal.
Hemorrhages located in other locations around the optic nerve are likely to be due to NGON or another cause, such as posterior vitreous detachment, retinal vascular disorders, anemia, hypertension, and ischemic optic neuropathy.9
After assessing the optic nerve, it can also be beneficial to look around the retina for any RNFL asymmetry and/or wedge defects, as these indicate either glaucoma or NGONs. An intact RNFL will display white streaks, both superior and inferior, in the temporal region. The density of these streaks can be compared while examining the fundus to identify signs of relative RNFL thinning or atrophy, which in a glaucoma patient can indicate glaucoma progression. If there is severe RNFL atrophy, wedge defects become noticeable. These defects appear as darkened areas. As a reminder, RNFL defects can also happen due to NGONs, so it is essential we consider the diagnosis in the context of the optic nerve appearance.
• RNFL and ganglion cell analysis (GCA). A glaucomatous RNFL thinning appears superior temporally (ST) and inferior temporarily (IT) vs. RNFL thinning nasally or at the maculopapular bundle. NGON RNFL changes can result in ST/IT thinning but can also involve the nasal and/or maculopapular bundle. If such RNFL changes are noticed, we should consider NGON as the diagnosis.
When looking at the GCA, the macular vulnerability zone, also known as the inferotemporal zone, becomes quite im- portant. If the IT fibers from the optic nerve, which should correlate with the inferior half of the macular GCA, are damaged, we are likely dealing with glaucoma.10 Often in glaucoma, the RNFL OCT defects follow its pattern onto the GCA, further solidifying glaucomatous damage and diagnosis.
In NGON, the thinning on GCA will often appear more diffuse and denser.
• Macular thickness. OCT shows that individuals who have a NGON have reduced macular thickness vs. those who have glaucoma. The theory for this finding is that NGON may be more preferential to the papillomacular bundle, resulting in greater macular involvement.11 Where glaucoma only involves the RNFL and ganglion cell layer, some NGON, such as central retinal artery occlusion/branch retinal artery occlusion, involve more retinal layers, resulting in a thinner retina. Incidentally, a decrease of ≥25 µm in the average intraocular macular thickness (ST vs. IT), and two blocks measuring ≤200 µm, suggest the possibility of an old branch retinal artery occlusion.12
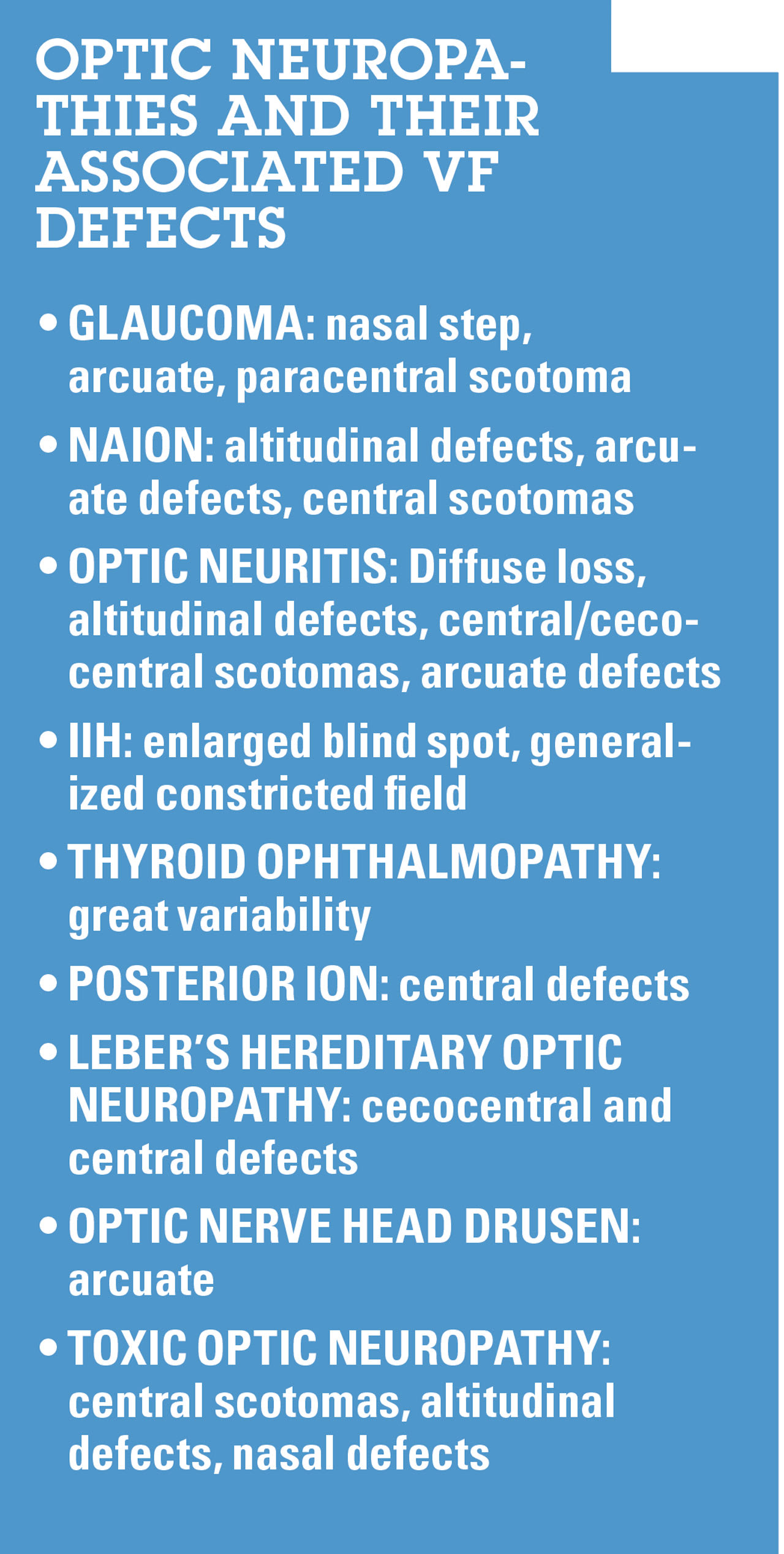
• VF. Glaucoma often exhibits arcuate scotomas, nasal steps, and paracentral scotomas. Notably, glaucomatous VF defects typically do not extend across the horizontal midline. Conversely, NGONs present with a variety of VF defects, such as enlarged blind spots, with central defects frequently observed.13-17 (See “Table 5: Optic Neuropathies and their Associated VF Defects.") If there is progressive VF decline despite well-controlled IOP, a neurologist consultation should be considered for neuroimaging of the patient.
Accurate diagnosis
This article offers a systematic approach for precise diagnosis, emphasizing meticulous case analysis, comprehensive symptom assessment, consideration of onset and progression, exploration of medical and family histories, scrutiny of medication factors, and thorough ocular evaluations. Additionally, it underscores the significance of modern diagnostic tools, such as OCT and VF testing. The integration of these tools with this systematic diagnostic approach increases the likelihood of an accurate diagnosis, ensuring patients receive the care needed to safeguard their ocular health. OM
References
- Le A, Mukesh BN, McCarty CA, Taylor HR. Risk factors associated with the incidence of open-angle glaucoma: the visual impairment project. Invest Ophthalmol Vis Sci. 2003;44(9):3783-9. doi: 10.1167/iovs.03-0077.
- Wu X, Konieczka K, Liu X, Chen M, Yao K, Wang K, Flammer J. Role of ocular blood flow in normal tension glaucoma. Adv Ophthalmol Pract Res. 2022;2(1):100036. doi: 10.1016/j.aopr.2022.100036.
- Ma KS, Lee CM, Chen PH, Yang Y, et al. Risk of Autoimmune Diseases Following Optic Neuritis: A Nationwide Population-Based Cohort Study. Front Med (Lausanne). 2022;9:903608. doi: 10.3389/fmed.2022.903608.
- Lachkar Y, Bouassida W. Drug-induced acute angle closure glaucoma. Curr Opin Ophthalmol. 2007;18(2):129-33. doi: 10.1097/ICU.0b013e32808738d5.
- Ocular Hypertension Treatment Study Group; European Glaucoma Prevention Study Group; Gordon MO, Torri V, Miglior S, et al. Validated prediction model for the development of primary open-angle glaucoma in individuals with ocular hypertension. Ophthalmology. 2007;114(1):10-9. doi: 10.1016/j.ophtha.2006.08.031.
- Mikolajczyk B, Ritter A, Larson C, et al. Red Desaturation Prevalence and Severity in Healthy Patients. Neurol Clin Pract. 2022;12(1):1-5. doi: 10.1212/CPJ.0000000000001011.
- Bengtsson B. The variation and covariation of cup and disc diameters. Acta Ophthalmol (Copenh). 1976;54(6):804-18. doi: 10.1111/j.1755-3768.1976.tb01801.x.
- Greenfield DS, Siatkowski RM, Glaser JS, Schatz NJ, Parrish RK 2nd. The cupped disc. Who needs neuroimaging? Ophthalmology. 1998;105(10):1866-74. doi: 10.1016/S0161-6420(98)91031-4.
- Razeghinejad MR, Nowroozzadeh MH. Optic disk hemorrhage in health and disease. SurvOphthalmol. 2017;62(6):784-802. doi: 10.1016/j.survophthal.2017.04.001.
- Hood DC, Raza AS, de Moraes CGV, Liebmann JM, Ritch R. Glaucomatous damage of the macula. Prog Retin Eye Res. 2013;32:1-21. doi: 10.1016/j.preteyeres.2012.08.003.
- Gupta PK, Asrani S, Freedman SF, et al. Differentiating glaucomatous from non-glaucomatous optic nerve cupping by optical coherence tomography. Open Neurol J. 2011;5:1-7. doi: 10.2174/1874205X01105010001.
- Sullivan-Mee M, Amin P, Pensyl D, Katiyar S. Differentiating Occult Branch Retinal Artery Occlusion from Primary Open-angle Glaucoma. Optom Vis Sci. 2018;95(2):106-112. doi: 10.1097/OPX.0000000000001170.
- Wall M, George D. Idiopathic intracranial hypertension. A prospective study of 50 patients. Brain. 1991;114 (Pt 1A):155-80. Link.
- Kedar S, Ghate D, Corbett JJ. Visual fields in neuro-ophthalmology. Indian J Ophthalmol. 2011;59(2):103-9. doi: 10.4103/0301-4738.77013.
- Keltner JL, Johnson CA, Spurr JO, Beck RW. Baseline visual field profile of optic neuritis. The experience of the optic neuritis treatment trial. Optic Neuritis Study Group. Arch Ophthalmol. 1993;(2):231-4. doi: 10.1001/archopht.1993.01090020085029.
- Hayreh SS, Zimmerman B. Visual field abnormalities in nonarteritic anterior ischemic optic neuropathy: their pattern and prevalence at initial examination. Arch Ophthalmol. 2005:1554-62. doi: 10.1001/archopht.123.11.1554.
- Hayreh SS. Posterior ischaemic optic neuropathy: clinical features, pathogenesis, and management. Eye (Lond). 2004;18(11):1188-206. doi: 10.1038/sj.eye.6701562.

Dr. Shah is the Ocular Disease Resident at Center for Sight, in Carmel, Ind.