

Geographic atrophy (GA) is the progressive, irreversible, advanced form of dry age-related macular degeneration (AMD). It is characterized by sharply demarcated atrophic lesions in the outer retina. In addition to atrophy of the retinal pigment epithelium (RPE), GA may include loss of overlying photoreceptors and underlying choriocapillaris (CC).1 Dysregulated activation of the complement system can lead to inflammation and cell death, resulting in the GA phenotype.1,2
The choroid nourishes the outer retina, and the RPE depends on the CC for survival. The choroid also supplies the foveal avascular zone, which lacks retinal blood vessels. Pathologic changes in outer retinal perfusion may be a significant early contributing factor to AMD.2 The choroid has been implicated in the inflammation and complement activation in AMD, with disproportionate accumulation of the membrane attack complex in the CC, as well as mast cell and macrophage activation.1,2
Atrophic lesions can invade the fovea in less than 2 years from the point at which they form in the non-subfoveal retina.2 Therefore, early intervention preceding foveal involvement may slow lesion growth and preserve vision over the long term. Complement inhibition has been identified as a key avenue for therapeutic intervention.1
Never has the choroid been more accessible. With the emergence of fundus autofluorescence (FAF), near infrared (NIR), enhanced-depth imaging optical coherence tomography (EDI-OCT), swept-source OCT (SS-OCT), and OCT-angiography (OCTA), clinicians have discovered a new frontier of insights related to physiological and pathological features of choroidal morphology.2,3
Choriocapillaris Degeneration in Geographic Atrophy
Early AMD is characterized by several changes, including the onset of degeneration of the CC.4 While some choroidal atrophy is expected with age, the amount of CC atrophy in AMD far exceeds the amount attributable to normal aging.5,6 Even at early stages of AMD, CC dropout has been observed.6
Seddon et al found CC dropout was present in early AMD samples, even below areas of intact RPE.6 Seddon found higher CC vascular loss for all stages of AMD compared to controls. In early and intermediate AMD, 20.5% and 12.5% loss of CC vascular area was seen, respectively, and a 39.0% loss was seen in GA.6 “Ghost vessels” were identified in AMD eyes. These represent the remains of previously healthy CC that have lost their endothelia.
In healthy eyes, choroidal thickness should approach that of the retina. In patients with early AMD, several studies have shown a significantly higher degree of choroidal thinning in eyes with reticular pseudodrusen (RPD) compared to those without.2,7,8 Other OCT studies revealed similar choroidal thinning in advanced dry AMD. 2,9.10 In patients with GA, OCTA has demonstrated dramatic thinning of the CC at the areas of RPE atrophy.9,10 OCTA has further corroborated the choroidal attenuation seen on histopathology and OCT.
Sohn and colleagues found that VEGF-A levels were negatively correlated with CC vascular density.3 These findings support the thinking that choroidal vascular degeneration, predominantly in the CC, contributes to dry AMD progression and GA.3 Addressing choroidal microvasculature loss in AMD remains an important translational target.
The choroid plays a critical role in the pathogenesis of GA by being a site of atrophy and a potential contributor to the progression of the disease.
Key Clinical Takeaways
- AMD has traditionally been viewed as a disease with primary origins related to damage to the RPE.
- While the bulk of AMD research rightfully focuses on the role of the RPE, the importance of the choroid cannot be overlooked.
- The choroid has been implicated in the inflammation and complement activation in AMD.
- Histopathologic and OCTA studies have demonstrated that choroidal vascular depletion is present in early disease and is progressive in GA and neovascular AMD phenotypes.
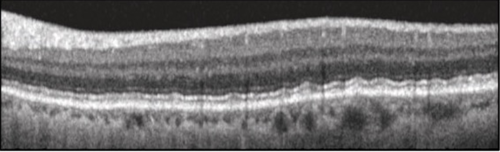
Figure 1. "Leptochoroid" refers to a thin choroid, as seen here. This is a 69-year-old male with early AMD.
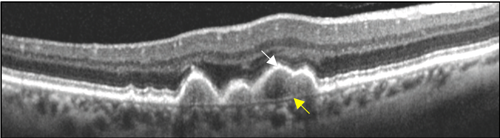
Figure 2. Thinning of the choroid in an eye with confluent drusen. Note ellipsoid zone (EZ) band dropout overlying the soft drusen (white arrow) and visibility of Bruch membrane (yellow arrow).



Figure 3. Multimodal imaging of an eye with GA and 20/400 VA. Note the visible choroidal vessels within the area of GA (A, black arrow). NIR imaging defines the GA boundaries (B, blue arrows). In the OCT horizontal B-scan through the GA lesion (C), note the enhanced signal from the central choroid due to overlying RPE/PR atrophy (red arrow). The ELM and EZ band are not visible between the purple arrows.




Figure 4. Multimodal imaging of an eye with GA and 20/60 VA. Note refractile drusen and areas of central macular thinning (A). FAF shows patches of hypo- and hyper-AF, correlating to RPE cell death and adverse metabolic activity, respectively (B). In this NIR + OCT horizontal B-scan (C and D), note that the foveal retina is thinned. Loss of outer retinal layers and RPE is moderate and localized, as is choroidal enhancement. This patient is receiving monthly intravitreal complement inhibition pharmacotherapy.
References
- Bakri SJ, Bektas M, Sharp D, Luo R, Sarda SP, Khan S. Geographic atrophy: Mechanism of disease, pathophysiology, and role of the complement system. J Manag Care Spec Pharm. 2023;29:S2–S11. doi:10.18553/jmcp.2023.29.5-a.s2
- Farazdaghi MK, Ebrahimi, KB. Role of the choroid in age-related macular degeneration: A current review. J Ophthalmic Vis Res. 2019;14:78. doi:10.4103/jovr.jovr_125_18
- Sohn, EH, Flamme-Wiese, MJ, Whitmore, SS et al. Choriocapillaris degeneration in geographic atrophy. Am J Pathol. 2019;189:1473–1480. doi:10.1016/j.ajpath.2019.04.005
- Chirco KR, Sohn EH, Stone EM, Tucker BA, Mullins RF. Structural and molecular changes in the aging choroid: Implications for age-related macular degeneration. Eye (Lond). 2017;31:10–25. doi:10.1038/eye.2016.216
- Wakatsuki Y, Shinojima A, Kawamura A, Yuzawa M. Correlation of aging and segmental choroidal thickness measurement using swept source optical coherence tomography in healthy eyes. PLoS One. 2015;10:e0144156. doi:10.1371/journal.pone.0144156
- Seddon JM, McLeod DS, Bhutto IA, et al. Histopathological insights into choroidal vascular loss in clinically documented cases of age-related macular degeneration. JAMA Ophthalmol. 2016;134:1272–1280. doi:10.1001/jamaophthalmol.2016.3519
- Garg A, Oll, M, Yzer, et al. Reticular pseudodrusen in early age-related macular degeneration are associated with choroidal thinning. Invest Ophthalmol Vis Sci. 2013;54:7075–7081. doi:10.1167/iovs.13-12474
- Yun C, Ahn J, Kim M, Hwang SY, Kim SW, Oh J. Ocular perfusion pressure and choroidal thickness in early age-related macular degeneration patients with reticular pseudodrusen. Invest Ophthalmol Vis Sci. 2016;57:6604–6609. doi:10.1167/iovs.16-19989
- Sigler EJ, Randolph JC, Calzada JI, Charles S. Smoking and choroidal thickness in patients over 65 with early-atrophic age-related macular degeneration and normals. Eye (Lond). 2014;28:838–846. doi:10.1038/eye.2014.100
- Spaide R F. Age-related choroidal atrophy. Am J Ophthalmol. 2009;147:801-810. doi:10.7150/ijbs.49890


This editorially independent content is sponsored by ![]()