


This is the second in a series focusing on the diagnosis and treatment of geographic atrophy.
Geographic atrophy (GA), an advanced form of dry age-related macular degeneration (AMD), is on the rise. More than 1 million people in the United States and about 1 in 5 people worldwide (8 million) are living with GA. 1, 2, 3 GA is irreversible, progresses faster than previously thought, and accounts for approximately 20% of legal blindness.4, 5 Considering this, it is imperative to detect GA early, monitor closely, and refer promptly for intervention with intravitreal complement inhibition pharmacotherapy.
GA is characterized by accumulation of drusen, loss of photoreceptor cells, retinal pigment epithelium (RPE) changes, and retinal and choroidal atrophy leading to distinct atrophic lesions in the macula, which tends to increase with time.6 From the initial GA diagnosis, it takes an average of 2 years for patients to experience significant vision impairment as the atrophic lesions invade the fovea.7, 8, 9
With increased prevalence and rate of progression, as well available options for intervention, it is increasingly important that optometrists are confident and comfortable in taking at least these 3 steps to support patients at risk for or living with GA.
- Raise awareness: Risk factors for GA include advanced age, race (Caucasians), family history, genetics (complement factor H —CFH). Encouraging lifestyle changes including smoking cessation (including e-cigarette use or vaping), adopting a healthy diet, and managing weight can slow down GA progression.
- Multimodal imaging: This provides anatomic insight of the retina and choroid and detection of biomarker features that improve early detection, staging, monitoring, and therapeutic interventions in GA.9 Multimodal imaging including color fundus images (CFP), fundus autofluorescence (FAF), near-infrared (NIR), enhanced-depth imaging optical coherence tomography (EDI-OCT), optical coherence tomography (OCT), and optical coherence tomography angiography (OCTA) may detect early biomarkers of GA.
- Timely referrals: Timely referral is crucial. With the availability of intravitreal complement inhibition pharmacotherapy, early intervention can stabilize vision and slow disease progression.
By prioritizing education, leveraging advanced diagnostics, and ensuring timely referrals, eyecare providers can make a significant difference in preserving vision and improving patients' quality of life in patients with GA.
Key Clinical Takeaways
- Geographic atrophy (GA) is on the rise as the population ages.
- Education is crucial. Helping patients recognize the impact of their choices empowers them to take preventive action.
- Multimodal imaging is critical in detecting subclinical changes and key biomarker features before symptoms manifest.
- All patients who are at risk for GA should be made aware of options that could slow down the progression.
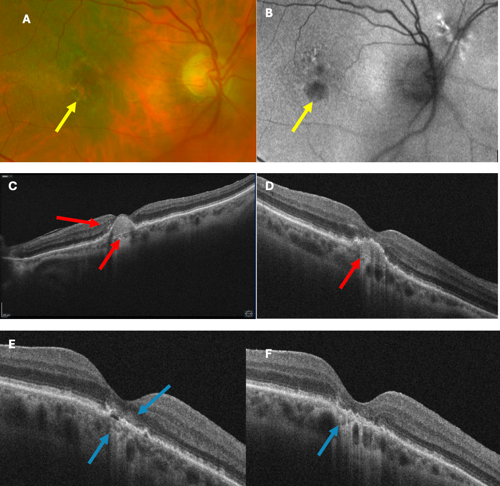
Figure 1. Multimodal imaging of an 85-year-old Caucasian female with GA in her right eye and BCVA of 20/40. (A) Color fundus images (CFP) revealed an extrafoveal GA lesion, (B) fundus autofluorescence (FAF) show hypo-AF of the lesion indicating RPE cell death (yellow arrows). (C) OCT testing revealed a large drusenoid pigment epithelial detachment (PED) with retinal pigment epithelium (RPE) pigment migration and visibility of Bruch membrane (red arrow).
At 2 to 3 years follow-up, OCT biomarkers for GA progression with (D) softening of PED and overlying RPE disruption (red arrows), (E) collapse of PED with incomplete RPE and outer retinal atrophy (iRORA) - hypertransmission defects and subsidence (sinking) of the inner nuclear layer (INL) and outer plexiform layer (OPL) and hyporeflective wedges (blue arrow), and (F) progression of hypertransmission defect towards cRORA (complete RPE and outer retinal atrophy). Patient was referred for complement inhibitor intervention.
References
- Saundankar V, Borns M, Broderick K, et al. Annual prevalence of geographic atrophy and wet age-related macular degeneration among Medicare Advantage enrollees in a US health plan. J Manag Care Spec Pharm. 2025;31(1):88–94. doi:10.18553/jmcp.2025.31.1.88
- Rein DB, Wittenborn JS, Burke-Conte Z, et al. Prevalence of age-related macular degeneration in the US in 2019. JAMA Ophthalmol. 2022;140(12):1202–1208. doi:10.1001/jamaophthalmol.2022.4401
- Kalpana R, Farokh D, Arun U. Geographic atrophy: pathophysiology and current therapeutic strategies. Ophthalmol. 2023; 3:1327883. doi:10.3389/fopht.2023.1327883
- Fleckenstein M, Mitchell P, Freund KB, et al. The progression of geographic atrophy secondary to age-related macular degeneration. Ophthalmol. 2018;125(3):369–390. doi:10.1016/j.ophtha.2017.08.038
- Holz FG, Strauss EC, Schmitz-Valckenberg S, van Lookeren Campagne M. Geographic atrophy: clinical features and potential therapeutic approaches. Ophthalmol. 2014; 121(5): 1079–1091. doi:10.1016/j.ophtha.2013.11.023
- Farazdaghi MK, Ebrahimi, KB. Role of the choroid in age-related macular degeneration: A current review. J Ophthalmic Vis Res. 2019; 14:78. doi:10.4103/jovr.jovr_125_18
- Keenan TD, Agrón E, Domalpally A, et al. Progression of geographic atrophy in age-related macular degeneration: AREDS2 report number 16. Ophthalmol. 2018 Dec; 125(12):1913–1928. doi:10.1016/j.ophtha.2018.05.028
- Lindblad AS, Lloyd PC, Clemons TE, et al. Change in area of geographic atrophy in the age-related eye disease study: AREDS report number 26. Arch Ophthalmol. 2009 Sep;127(9):1168–1174. doi:10.1001/archophthalmol.2009.198
- Pfau M, Künzel SH, Pfau K, Schmitz-Valckenberg S, Fleckenstein M, Holz FG. Multimodal imaging and deep learning in geographic atrophy secondary to age-related macular degeneration. Acta Ophthalmol. 2023;101(8):881–890. doi:10.1111/aos.15796
Acknowledgement: Dr. Murry Falkner, Nova Southeastern University College of Optometry Ocular Disease Resident


This editorial content was supported via unrestricted sponsorship