


With two complement inhibitors now approved specifically for geographic atrophy (GA) secondary to age-related macular degeneration (AMD), it is imperative to identify patients with this disease. Both treatments slow the progression of GA when administered either monthly or every other month and potentially allow patients more time with functional vision.
The definition of GA has historically been based on its clinical appearance of well-defined regions of retinal pigment epithelium (RPE) atrophy with increased visibility of the underlying choroid, specifically in the setting of advanced stage non-exudative AMD.
More recently, the Classification of Atrophy Meeting coined optical coherence tomography (OCT) based terminology—including the terms complete RPE and outer retinal atrophy (cRORA) to describe GA seen on OCT. The OCT criteria for cRORA is “(1) a region of hypertransmission of at least 250 μm in diameter, (2) a zone of attenuation or disruption of the RPE of at least 250 μm in diameter, (3) evidence of overlying photoreceptor degeneration, and (4) absence of scrolled RPE or other signs of an RPE tear.”1
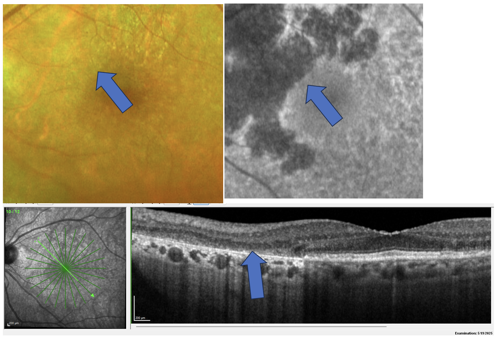
In addition, it is now widely accepted that GA may be difficult to identify on clinical examination alone. Ancillary testing such as OCT and fundus autofluorescence increase its visibility and make for an easier diagnosis (Figure 1).1
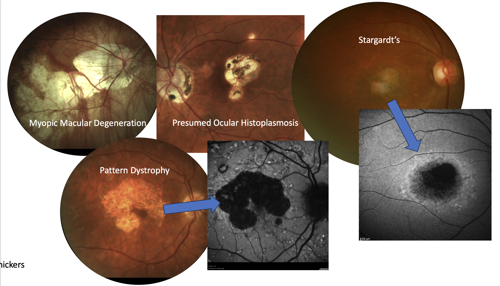
Even still, it is crucial to note that AMD is not the only disease that causes geographic regions of RPE and outer retinal atrophy. This finding can be seen in many pathological states that affect the outer retina including myopic macular degeneration and inherited retinal diseases such as Stargardt’s, pattern dystrophies, toxic maculopathies, macular telangiectasia type 2, infections, and others (Figure 2).
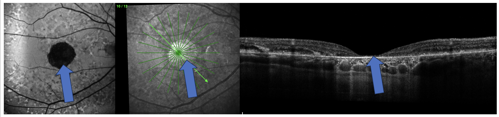
Just as multimodal imaging can help identify GA in the setting of AMD, it can also help to ensure that the condition being managed is truly AMD and not a masquerading condition. Fundus autofluorescence is especially helpful in noticing patterns of RPE atrophy or disruption that are not consistent with AMD (Figure 3).
Why is it so important to rule out non-AMD causes of outer retina atrophy? Current treatments are only approved for GA secondary to AMD. At this time, it is not known if they would have benefits in other conditions. As such, they should not be used for non-AMD diagnoses. Research does continue to see if intravitreal complement inhibitors would be helpful in other conditions, such as Stargardt’s disease.2
References
- Sadda SR, Guymer R, Holz FG, et al. Consensus definition for atrophy associated with age-related macular degeneration on OCT: Classification of Atrophy Report 3. Ophthalmology. 2018;125(4):537-548. doi:10.1016/j.ophtha.2017.09.028
- Stargardt disease research advances. Fighting Blindness Foundation. October 24, 2025. https://www.fightingblindness.org/news/stargardt-disease-research-advances-862

This editorial content was supported via unrestricted sponsorship