

A 75-year-old female patient presented for re-evaluation of intermediate age-related macular degeneration (AMD). She had noticed a bit more distortion in her vision OS since her last visit 6 months prior. She had been diagnosed with non-exudative macular neovascularization (NE-MNV) approximately 4 years ago and was typically seen every 6 months in clinic for dilation as well as optical coherence tomography (OCT) and OCT-angiography (OCT-A).
The patient utilizes home monitoring with ForeseeHome (FSH) technology (Notal Vision) to monitor her vision between office visits. She reported compliance with home monitoring and AREDS 2 supplements. No recent alerts were noted. Ocular history was remarkable for previous cataract surgery OU. Medical history was remarkable for type 2 diabetes, diagnosed approximately 20 years ago, with no history of diabetic retinopathy.
Visual acuity was 20/20 OD and 20/30 OS. This was stable compared to her last visit. Intraocular pressure was 12 mmHg OD and 14 mmHg OS via Goldmann applanation tonometry. Anterior segment examination revealed well-centered posterior chamber IOLs with trace posterior capsule opacification OU. Posterior segment examination showed medium and large drusen, RPE changes, and no evidence of fluid or hemorrhage OU. There was no evidence of diabetic retinopathy.
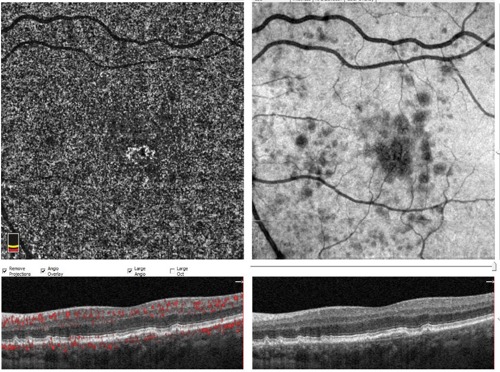

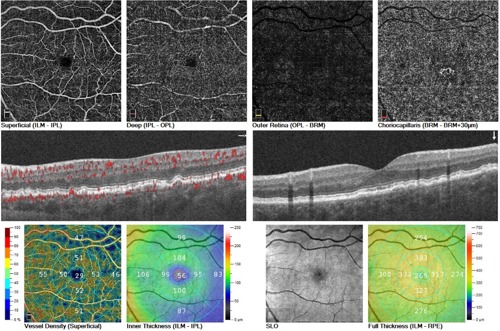
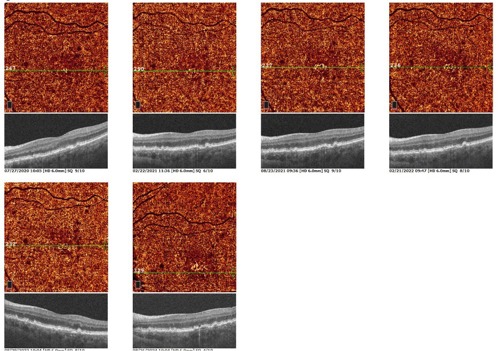
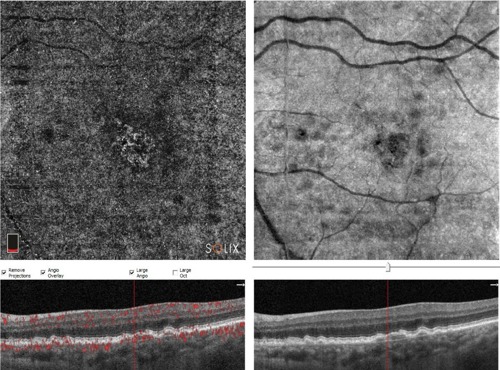
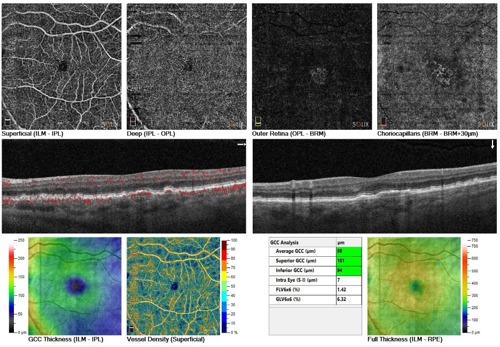
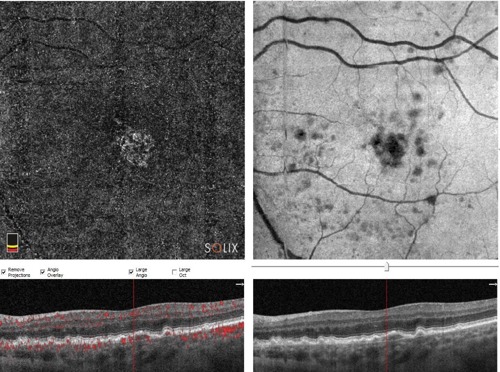
OCT and OCT-A were performed (Optovue Solix) to evaluate for signs of exudation OU and to assess the stability of her NE-MNV OS. No evidence of exudation or neovascularization was noted OD. OS showed stable drusen and a shallow retinal pigment epithelial detachment. OCT-A confirmed non-exudative CNV, slightly larger than previously noted. Of note, this was her first image on the Optovue Solix device. There was no evidence of intraretinal or subretinal fluid OS (Figures 5-7).
The patient was recommended to continue home monitoring and nutritional supplements. A follow-up appointment was scheduled for 6 months, sooner if new symptoms developed.
Non-exudative MNV usually refers to the entity of treatment naïve type 1 neovascularization in the absence of associated exudation.1 With OCT-A, there has been an ever-increasing appreciation of NE-MNV associated with AMD. The existing literature demonstrates that the presence of a newly diagnosed MNV in a non-exudative state represents a strong risk factor for future development of exudation, indicating the need for close monitoring after detection.
The mechanism of conversion from the non-exudative to the exudative stage of MNV is not completely understood. The 2-year cumulative exudation risk is 13.6 times greater in eyes with non-exudative MNV compared with eyes without detectable lesions, thus highlighting the importance of frequent monitoring in this population.2 Observation of NE-MNV is currently the recommended strategy, as anti-VEGF therapy should only be considered in cases with evidence of exudation (intraretinal and/or subretinal fluid).
This case demonstrates that NE-MNV may stay relatively stable for years. There is speculation that this may be a protective mechanism to reduce risk of geographic atrophy. When a new non-exudative lesion is detected, the follow-up interval should be decreased with more frequent examination and imaging. With chronic lesions, patients can be typically monitored every 4 to 6 months.
References
- Parravano M, Corradetti G, Cabral D, et al. Towards a better understanding of non-exudative choroidal and macular neovascularization. Prog Retin Eye Res. 2023 Jan; 92:101113.
- Yang J, Zhang Q, Motulsky E, et al. Two-year risk of exudation in eyes with nonexudative age-related macular degeneration and subclinical neovascularization detected with swept source optical coherence tomography angiography. Am J. Ophthalmol. 208. 1-11.

This editorial content was supported via unrestricted sponsorship.