

A 26-year-old male patient presented to the specialty contact lens clinic after completing corneal cross-linking in both eyes for treatment of progressive keratoconus. The patient had previously worn scleral lenses; however, they had been uncorrected for 2 years due to financial restrictions. Presenting uncorrected visual acuity was 20/80 in the right eye and 20/400 in the left eye with pin hole to 20/25 and 20/30 in the right and left eye, respectively. Refraction corrected the patient to 20/30 OD and 20/150 OS. Anterior segment examination revealed mild central corneal haze consistent with prior crosslinking along with Vogt’s striae in both eyes. No Muson’s or Rizzutti’s sign was present on examination.
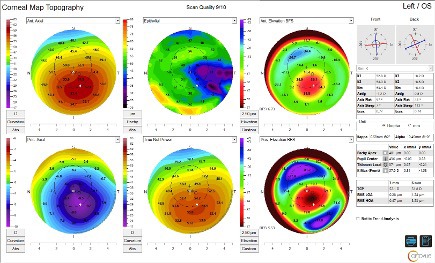
Topography (Optovue Solix, Visionix, USA) showed obvious signs of keratoconus including characteristic corneal thinning decentered inferior temporally with adjacent corneal steepening (see Figure 1). Evaluation of the surfaces of the cornea revealed more significant elevation on the posterior corneal surface than the anterior surface when compared to a best fit reference sphere. Most patients with keratoconus demonstrate epithelial remodeling, typically with thinning over the corneal apex surrounded by a ring of epithelial thickening. In this case, the patient showed that characteristic appearance, though the area of thinning was slightly decentered from the apex.
It was determined that a scleral contact lens would benefit this patient via probe lens testing. A diagnostic scleral lens was applied to each eye to assess for visual improvement. Scleral lens corrected visual acuity (VA) was 20/25 in both the right and left eyes, and the patient reported a reduction in distortions, halos, and starbursts around objects and lights. Due to the visual improvement and subjective aberration relief, scleral lens wear was recommended for both eyes; however, the patient could only afford one lens. Based on the magnitude of visual improvement in each eye between spectacle-corrected VA and scleral lens–corrected VA, it was determined that a lens would be more beneficial in the left eye than the right, and a fitting was initiated in the left eye only. A standard toric soft contact lens was trialed in the right eye, but the patient was concerned with the cost, as well as the stability of the lens with each blink. The patient was then prescribed spectacle lenses to wear over the scleral lens, which had his spectacle prescription in the right eye and a plano lens in the left.
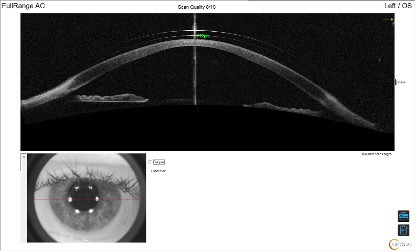
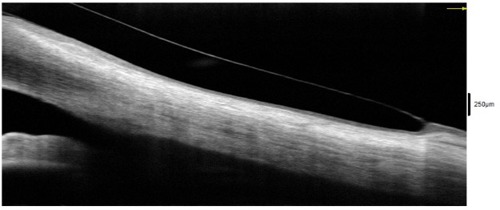
Based on the findings of a diagnostic scleral lens fitting, a trial lens was ordered. To improve the accuracy of the fit, anterior segment optical coherence tomography (OCT) technology (Optovue Solix, Visionix, USA) was utilized in conjunction with slit lamp examination to evaluate the central clearance, limbal clearance, and edge alignment. Slit lamp evaluation of the initial trial lens revealed an adequate central clearance with no areas of central touch, inferior decentration with thin limbal clearance superiorly and excessive limbal clearance inferiorly, and slightly flat edge alignment both temporally and superiorly. When evaluated via OCT imaging, the central clearance was measured to be 222 µm as seen in Figure 2. The superior limbal zone was clearing adequately, while the inferior limbal zone showed excessive clearance.
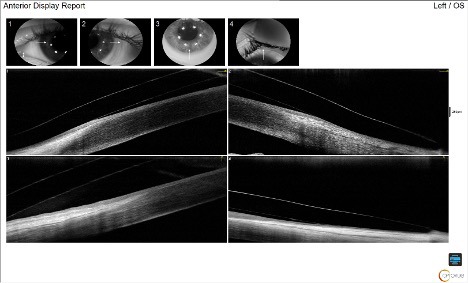
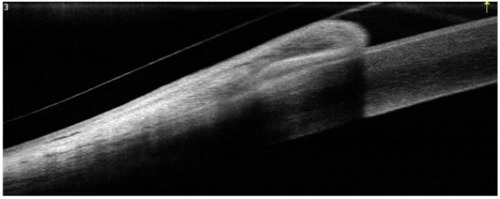
The excessive inferior clearance was not concerning, as there were no signs of conjunctival swelling or prolapse on OCT (see Figure 3) and no limbal hyperemia on slit lamp examination. Good edge alignment was found at 360º, showing conjunctiva covering half of the lens edge thickness on OCT. The trial was dispensed to the patient, and a follow-up exam was completed 1 week later. At the follow-up appointment, after 5 hours of lens wear, the central clearance was 205 µm, the limbal zone showed no change, and no conjunctival prolapse was found inferiorly in the area of excessive limbal clearance. The edge alignment was improved superiorly and temporally, no blanching was present on slit lamp evaluation, and the patient reported no foreign body sensation. The lens was removed, and sodium fluorescein stain was instilled. No staining or impression ring pooling were present on the cornea or conjunctiva. The scleral lens prescription was finalized, and the patient was instructed to return to care in 6 months for a scleral lens progress examination and possible fitting of the right eye.
Discussion
Anterior segment OCT can be an invaluable tool to assist with scleral lens fitting and improve lens accuracy and alignment. This straightforward scleral lens fitting case demonstrates the ease of scleral lens fitting with OCT assistance. Several Optovue Solix scan protocols can be useful, including Corneal Mapping (full corneal epithelial, stromal, and pachymetry mapping), to achieve corneal topography and select the initial diagnostic lens. FullRange AC, which can capture the entire anterior chamber in a single scan, can help image the central and limbal zones, and the Cornea Angle scan, which quantifies the openness of the iridocorneal angle, is useful for a more magnified limbal zone image as well as edge alignment.
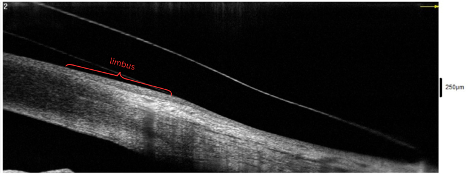
The ideal fit of a scleral lens shows a central clearance of around 200 µm, no limbal touch, and edge alignment with the sclera. On OCT, the limbus can be seen as a reflectivity change in the cornea (see Figure 4). This area should not be touched by the lens but should also not have excessive clearance, as negative pressure forces can pull the conjunctiva into that zone and cause conjunctival prolapse (see Figure 5) or excessive limbal hyperemia. OCT can also assist with evaluation of edge alignment. Appropriate edge alignment will be shown when the conjunctiva overlies half or more of the edge thickness, as seen in Figure 6, but does not fold over the edge of the lens.
Although scleral lens fitting without anterior segment OCT is possible, the process can be much more accurate and efficient with the addition of anterior segment OCT, specifically, the enhanced resolution and expanded width of scans, which allows for less image captures per eye. This is beneficial for reducing chair time, maximizing successful fitting within the warranty period, and increasing patient satisfaction by reducing their time in the office.
All images captured with the Optovue Solix (Visionix, USA), courtesy of Aubry Tackett, OD.
Disclaimer: The views and experiences expressed are those of the individual user. They may involve off-label use of the medical device, which is not endorsed or approved by the manufacturer.

This editorial content was supported via unrestricted sponsorship